
Inguinal Hernias

occur through the floor or the internal ring of the .
Epidemiology
- 75% of all hernias are inguinal.
- Men are 25 times more likely to have a hernia.
- The indirect variant is more common than the direct variant (2:1).
- Most commonly occur on the right side
- occurs in 1%–3% of all .
Classification
- Indirect:
- The hernia sac passes through the internal inguinal ring toward the external inguinal ring and into the .
- Frequently and associated with patent processus vaginalis
- Direct:
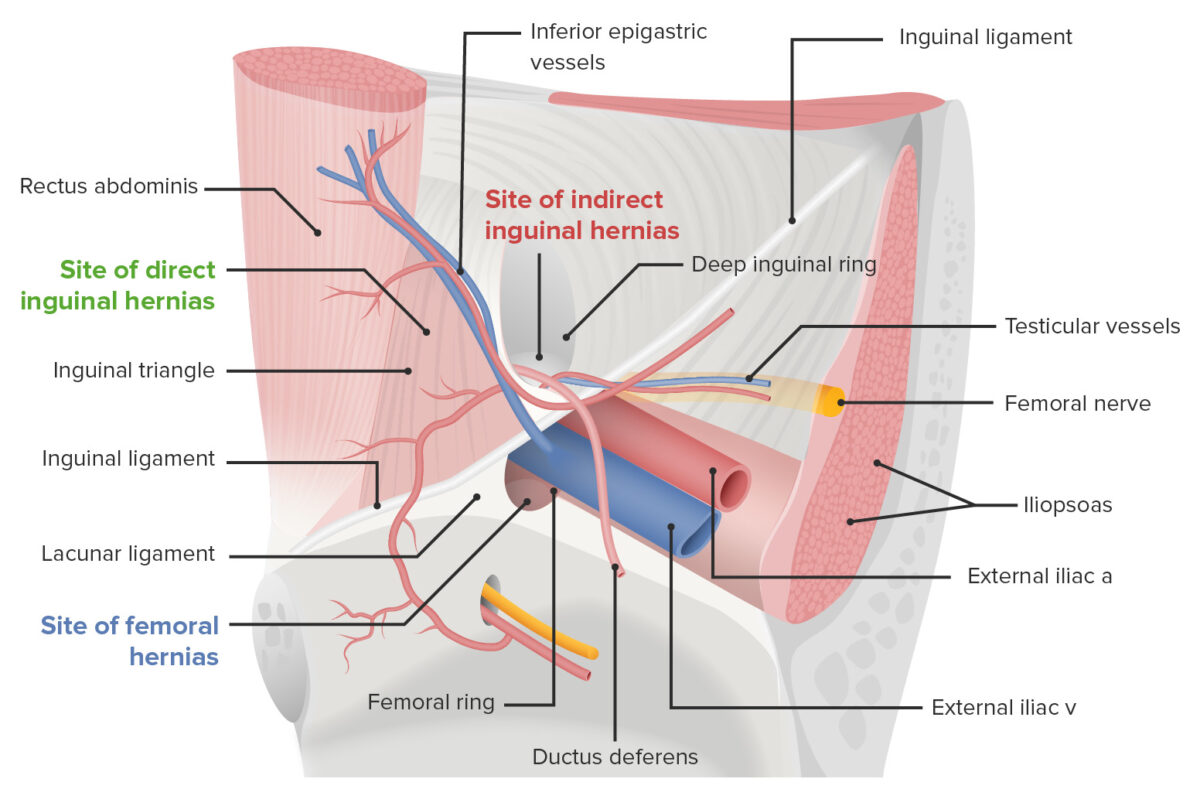
- The hernia sac protrudes anteriorly and is medial to the internal inguinal ring and inferior epigastric vessels.
- (site of direct ): formed by the , inferior epigastric vessels, and rectus sheath
- Mostly acquired secondary to muscular weakness and are more common in older men
- Combined (pantaloon): both indirect and direct hernia components

Surgical repair
Indications:
- or (emergent)
- Symptomatic hernia (associated with or discomfort)
Open approach:
- A transverse incision is made above the , which is at the midpoint between the and the pubic tubercle.
- The aponeurosis is incised, with care taken to identify the genital branch of the and the .
- The is mobilized and the hernia sac is dissected free.
- The contents of the hernia sac are reduced.
- The hernia sac can be reduced (direct), or the of the hernia sac can be ligated and excised (indirect).
- Primary repair () is rarely used nowadays as the failure rates are quite high.
- Options for :
- Bassini: approximation of the and the conjoint tendon ( aponeurosis) to the
- Shouldice:
- Layered repair
- Running suture to approximate the aponeurosis to the inguinal iliopubic tract
- Running suture to approximate the to the

- McVay:
- Interrupted, nonabsorbable suture to approximate the edge of the aponeurosis to Cooper’s ligament
- Cooper’s ligament and the are secured to the iliopubic tract.
- A relaxing incision is made in the anterior rectus sheath 1 cm above the pubic tubercle.

- Mesh repair:
- Lichtensteinrepair:
- A synthetic mesh with a slit in the middle is inserted into the canal to accommodate the and wrap around it.
- Using nonabsorbable suture, the mesh is secured to the pubic tubercle superiorly along the and inferiorly along the shelving edge of the .
- Plug and :
- A cone-shaped piece of polypropylene mesh is inserted into the internal ring.
- A flat piece of mesh is used to reinforce the floor of the similar to the process used in Lichtenstein repair.
- Lichtensteinrepair:
Laparoscopic approach:
- Always involves mesh placement
- Requires technical expertise
- Totally extraperitoneal (TEP) technique:
- Abdominal cavity is not entered.
- Dissection is performed in the preperitoneal space with a balloon and insufflation.
- Limited working space
- Transabdominal preperitoneal (TAPP) technique:
- Abdomen is entered using the open Hassan technique or Veress needle.
- is taken down and mesh is placed in the preperitoneal space.
- Larger working space
Complications:
- Chronic
- Testicular (damage to the testicular artery)
- (mesh )
- : of the testis due to viral or bacterial
- Seroma
- Scrotal

From a real surgery:





Ali Mardini
Hitta din inspiration till din framtid !